Most people have never heard of the psoas. That is worth changing, because if you have persistent lower back pain, hip tightness, or a sense of being physically braced even when nothing is actively threatening you, the psoas is very likely involved.
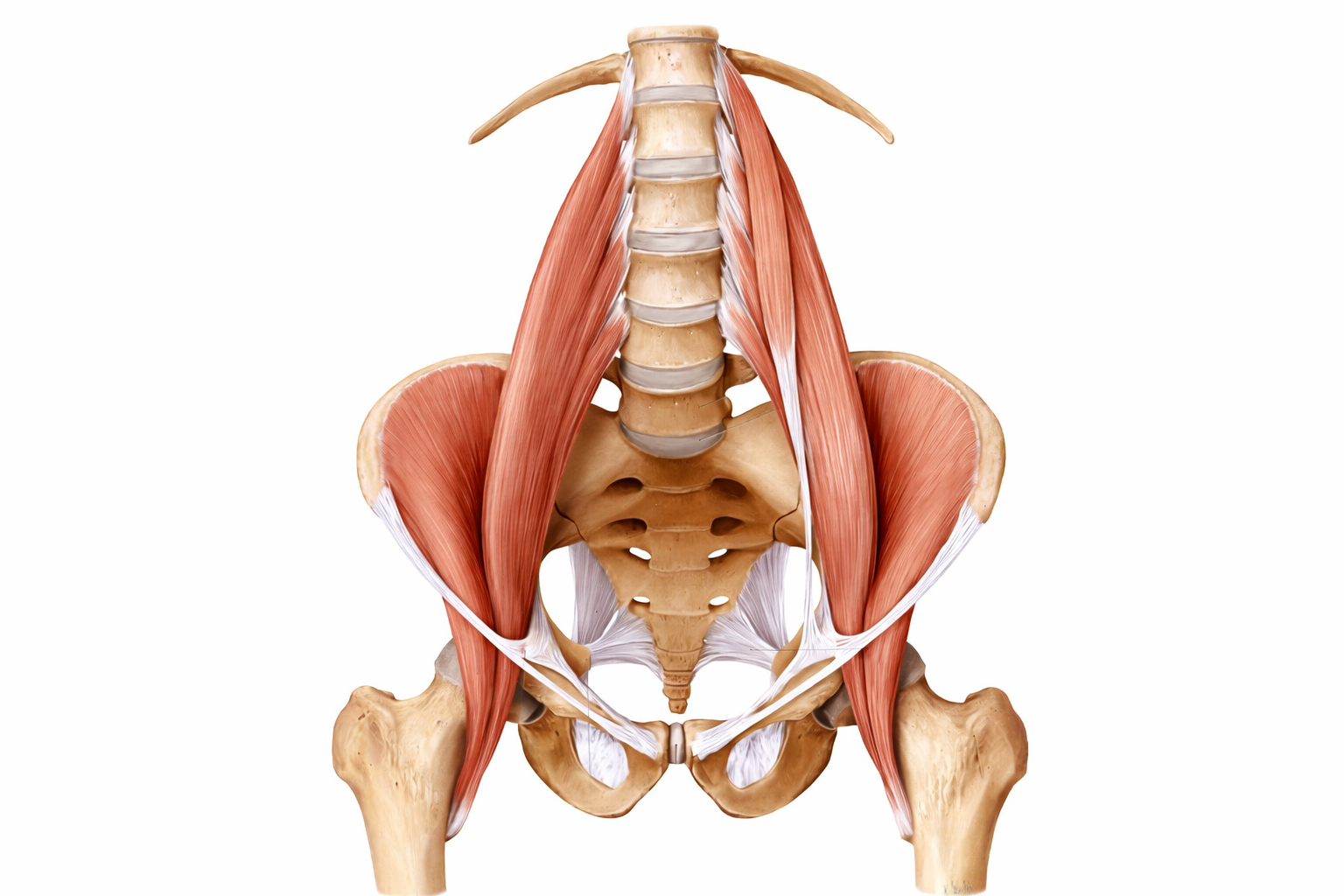
It is not a muscle you can see or feel easily from the outside. It sits deep in the abdomen, running from the sides of the lumbar vertebrae down through the pelvis to attach at the top of the inner thigh. It is the only muscle in the body with a direct structural connection between the spine and the leg. And it has a relationship with the nervous system that most back pain treatment never touches.
The psoas is not just a hip flexor. It is a postural muscle, a movement muscle, and a stress-response muscle. In chronic pain and chronic stress, all three of those roles become compromised at the same time.
Why the nervous system and the psoas are connected
The psoas is innervated by the lumbar plexus, a network of nerves emerging from the lower spine that overlaps significantly with the sympathetic nervous system. When the body enters a threat response, whether that threat is physical or psychological, the psoas is one of the first muscles to respond. It contracts, drawing the spine and the legs toward each other. This is the physical expression of the bracing pattern you see in a person who is frightened or preparing for impact.
In a genuine physical emergency, this makes sense. The body is preparing to run, to curl, to protect its vital organs. The problem is that the nervous system cannot reliably distinguish between a physical threat and a sustained psychological one. Work pressure, financial stress, unresolved conflict, chronic pain itself: all of these can keep the sympathetic nervous system in a low-level activated state, and the psoas responds accordingly. It stays shortened. The brace never fully releases.
Over weeks and months, the body stops being a place you live in and starts being a place you brace in. The psoas is where that distinction becomes structural.
Over weeks and months, this shows up in the body in predictable ways: an increased lumbar curve, a forward tilt of the pelvis, compression at the lower lumbar discs and facet joints, and a hip that never quite opens fully. The person is not doing anything wrong. Their nervous system is doing exactly what it was designed to do. But it is doing it continuously, without the off-switch.
What it does to the spine
Pulls the lumbar vertebrae forward and downward, increasing disc compression and facet joint load. Contributes to the anterior pelvic tilt seen in chronic lower back pain.
What it does to movement
Restricts full hip extension, altering walking mechanics and placing compensatory load on the sacroiliac joint, the hip rotators, and the thoracolumbar fascia.
What it does to breathing
The psoas and diaphragm share fascial continuity at the lumbar spine. A braced psoas restricts diaphragm movement, reinforcing the shallow breathing pattern that keeps the nervous system alert.
What it does to rest
Maintained tension in the psoas during sleep prevents full parasympathetic recovery. Many people wake stiff and compressed because the psoas never had the conditions to release overnight.
The diaphragm connection
This is the part most people find surprising. The psoas and the diaphragm are physically connected through the arcuate ligaments at the top of the lumbar spine. They share fascial tissue. They move together.
What this means in practice is that every breath you take influences the psoas, and the state of the psoas influences your breathing. A tight, braced psoas limits how far the diaphragm can descend on the inhale. This pushes the breathing pattern upward into the chest and neck, which is exactly the pattern that keeps the sympathetic nervous system active. The tight psoas and the restricted breath reinforce each other in a loop that neither stretching nor breathing alone fully resolves.
This is why the most effective approach to psoas release combines nervous system regulation with tissue work. The psoas does not respond well to force. Aggressive stretching of a muscle contracted as a protective response tends to produce more guarding, not less. The body needs to feel safe before the muscle will let go.
The psoas releases when the nervous system feels safe enough to allow it. Trying to force the release while the body is still braced produces more tension, not less. Ease always precedes release.
Why conventional hip flexor stretches often miss it
The standard kneeling hip flexor stretch, one knee down, hips forward, is a reasonable stretch for the iliacus and the rectus femoris. These are front-of-hip muscles that do need attention. But the psoas major, the deep portion that attaches to the lumbar vertebrae, is rarely reached by this position.
To access the psoas effectively you need positioning that allows the muscle to lengthen without triggering a guarding response, and a nervous system state calm enough to permit that lengthening. That combination is why the supported release positions below tend to produce results that the standing stretch does not.
The practice: two parts
The myofascial component works the fascia and musculature surrounding the psoas attachment point, particularly around the anterior hip crease and the lateral lower abdomen. The psoas itself is too deep for direct external access, but the surrounding structures respond well to sustained, gentle pressure from a firm ball. Size matters here: a ball of around four inches in diameter sits against the tissue at the right depth without creating sharp point-pressure that causes the body to guard rather than release.
Part one: the supported psoas release
- 1Lie on your back with knees bent, feet flat on the floor. Place a folded blanket under your head if needed. Let your lower back settle toward the floor without forcing it.
- 2Allow one knee to slowly fall out to the side, foot still on the floor. You are not forcing the hip open. You are removing the support and letting gravity do the work. If this produces any sharp sensation, bring the knee back toward centre slightly.
- 3Breathe slowly through the nose, long exhale. With each exhale, notice whether the hip settles a little further without effort. Stay for eight to ten slow breaths. The release, if it comes, will feel like a gentle softening rather than a stretch.
- 4Bring the knee back to centre slowly and repeat on the other side. You may notice one side is considerably tighter. This is common and often corresponds to the side of greater habitual stress or loading.
Part two: ball release at the hip attachment
- 1Lie face down on a comfortable surface. Place a firm four-inch ball in the crease where your hip meets your lower abdomen, slightly to the inside of the hip bone. This is the anterior hip, not the outer hip.
- 2Rest your weight gently onto the ball. You are not pressing into it. You are allowing your body weight to create the contact. If the sensation causes you to hold your breath, reposition the ball slightly outward or reduce the weight on it.
- 3Breathe slowly and stay still for 60 to 90 seconds. The tissue will begin to soften with sustained, gentle pressure. Stillness and breath do the work.
- 4Slide the ball slightly toward the inner thigh and hold again. This works the area where the psoas attaches to the femur. Same rule: weight, not force, and slow breath throughout.
- 5Repeat on the other side. Two minutes per side is sufficient. Follow with the supported release from part one if you have time.

What to notice afterward
After a psoas release practice, most people notice one or more of the following: a sense of length through the front of the hip, a slightly flatter lower back when standing, a spontaneous deeper breath, and occasionally a brief emotional response. That last one surprises people. The psoas has been described by some researchers as a storage site for habitual tension patterns, and releasing it can sometimes produce a momentary feeling of relief that goes beyond the physical. This is not unusual and is not something to be concerned about.
What you are unlikely to notice immediately is a complete resolution of lower back pain. The psoas responds to sustained, consistent work and to a nervous system that is gradually becoming less reactive. One session shifts things. Regular sessions, combined with the nervous system regulation practices we have been building across the past few weeks, change them.
Five minutes, three times a week, done consistently over a month will produce more change in a chronically tight psoas than an occasional deep session. The muscle is responding to a chronic pattern. It needs a consistent counter-signal, not a single correction.